Recent Posts



What Providers Mean by “First-Degree Relative” When Discussing Health Risk

When healthcare providers ask about your family medical history, the phrase “first-degree relative” often comes up. Patients may wonder why the question is asked, what counts as first-degree and why some relatives seem to matter more than others.
Family history is not about predicting illness with certainty. Some conditions are closely tied to genetics, while others are influenced more by lifestyle or environmental factors, making family history relevant but not determinative.
It is a tool providers use to better understand risk patterns, guide screening decisions and focus preventive care.
Degree of Relation Defined in Practical Terms
Healthcare providers typically group family history by degree of relation, which reflects how closely related someone is genetically.
First-degree relatives include parents, full siblings and children. These relatives share about half of your genetic material and often a similar environment.
Second-degree relatives include grandparents, aunts, uncles, nieces, nephews and half-siblings. These relatives share less genetic overlap but can still provide useful context.
Third-degree relatives include cousins and great-grandparents. Their health history usually carries less direct weight but can still help identify broader patterns.
This structure helps providers quickly assess how strongly a condition may be connected to inherited or shared risk factors.
How Family Relationships Matter Differently for Different Conditions
Not all conditions use family history in the same way. Some illnesses are more strongly influenced by genetics, while others are shaped by behavior, environment or aging. For example:
- Certain cancers are closely tied to inherited risk and benefit from early screening if a first-degree relative was affected.
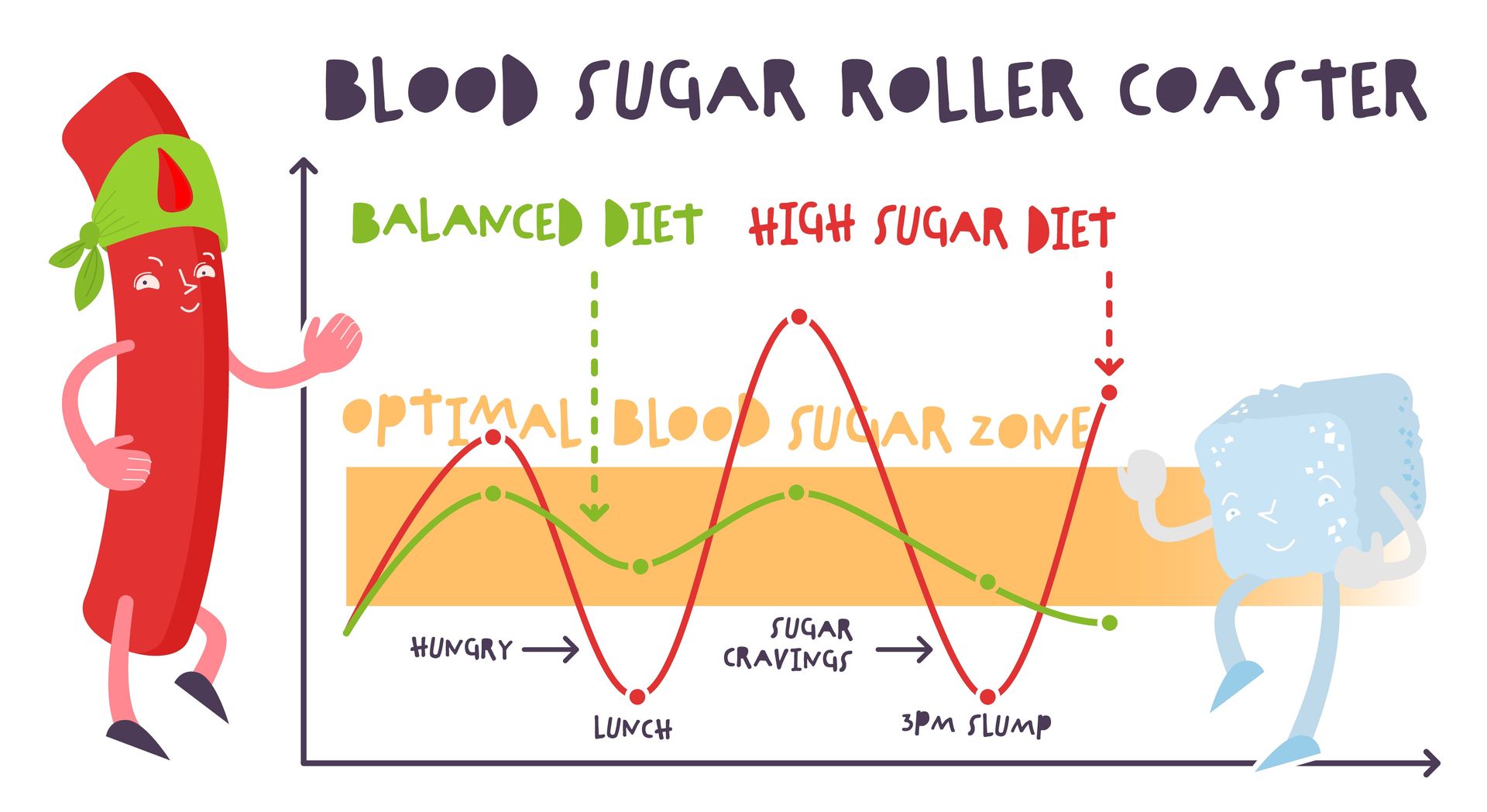
- Heart disease reflects both genetic predisposition and shared lifestyle factors.
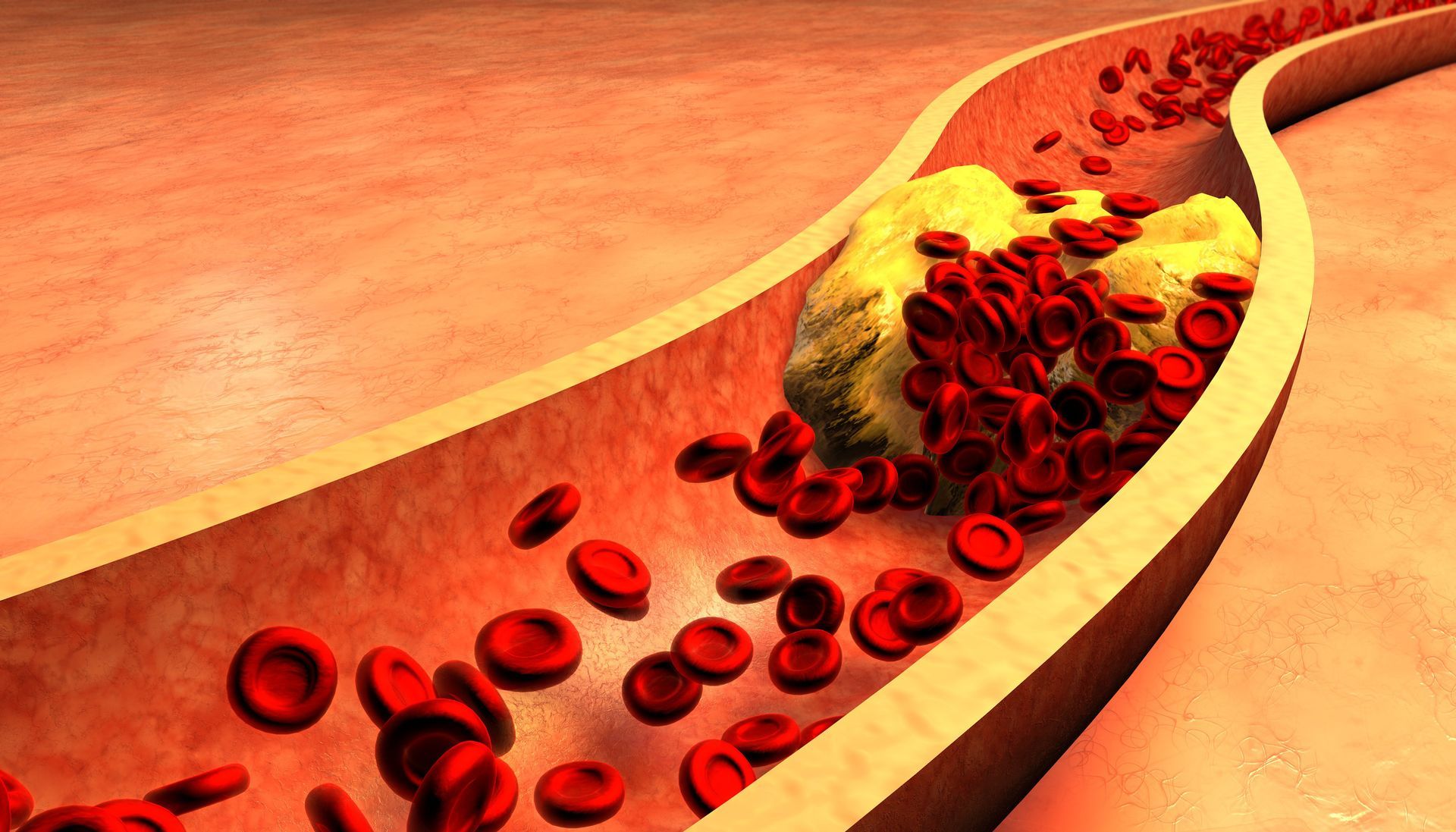
- Diabetes may cluster in families due to a combination of genetics, diet and activity patterns.
- Autoimmune conditions may appear across relatives without following a clear inheritance pattern.
Providers adjust how they interpret family history based on the condition being discussed.
This is why some questions feel more detailed for certain health topics than others.
Why Providers Ask “How Old Were They?”
Age of diagnosis often matters more than the diagnosis itself. When a condition appears earlier than expected, it can signal a stronger inherited component.
A single first-degree relative diagnosed at a young age may outweigh several relatives diagnosed later in life. For example, one parent diagnosed with heart disease at 45 may be more clinically relevant than multiple grandparents diagnosed in their 70s or 80s.
Early-onset disease suggests that genetics or shared risk factors may play a larger role.
Providers use this information to determine whether earlier screening or closer monitoring is appropriate.
When Second-Degree Relatives Become Important
Second-degree relatives matter when patterns emerge. If multiple second-degree relatives on the same side of the family have the same condition, providers may see this as a meaningful trend.
Second-degree history can also be important when first-degree information is incomplete rather than fully unavailable. In these situations, patterns among grandparents, aunts, uncles or cousins may provide useful context.
The Role of Third-Degree Relatives
Third-degree relatives generally have less influence on individual risk assessments, but they are not ignored entirely. Their history can add context, especially when conditions appear across multiple generations or cluster within one side of the family.
Third-degree information may be more relevant for rare conditions or when combined with first- and second-degree patterns. Providers use it to complete the picture rather than to drive decisions on its own.
How Providers Actually Use Family History
Family history is not used as a standalone diagnostic tool. Providers combine it with personal health history, physical exams, lab results and lifestyle factors. In practice, family history helps providers:
- Decide when to start or adjust screening
- Identify which risks deserve closer attention
- Focus preventive counseling on relevant areas
- Avoid unnecessary testing when risk is low
This approach is nuanced and individualized. Providers are not counting relatives as a checklist but evaluating the overall pattern.
What If You Do Not Know Your Full Family History?
Many patients simply do not have access to complete information. Partial details are still useful. Sharing what you know, even if timelines or diagnoses are unclear, helps providers make better-informed decisions.
Mentioning whether conditions occurred early or late, whether they were widespread or isolated, and which side of the family they came from can all be helpful.
Talk With Primary Care Providers in Houston About Your Family Health History
St. Hope Healthcare offers patient-centered care focused on understanding risk, supporting prevention and guiding informed health decisions.
Contact us by calling (713) 778-1300 to discuss your family medical history and develop a care plan tailored to your needs and goals.